
It can take five to 12 years for someone with clear endometriosis symptoms to receive a real diagnosis.
This might sound like a fringe data point, but it’s a professional assessment from Dr. Hugh Taylor, a reproductive endocrinologist at Yale and one of the leading researchers in the field. He finds that endometriosis is almost routinely dismissed; nearly every patient Dr. Taylor sees shares that experience.
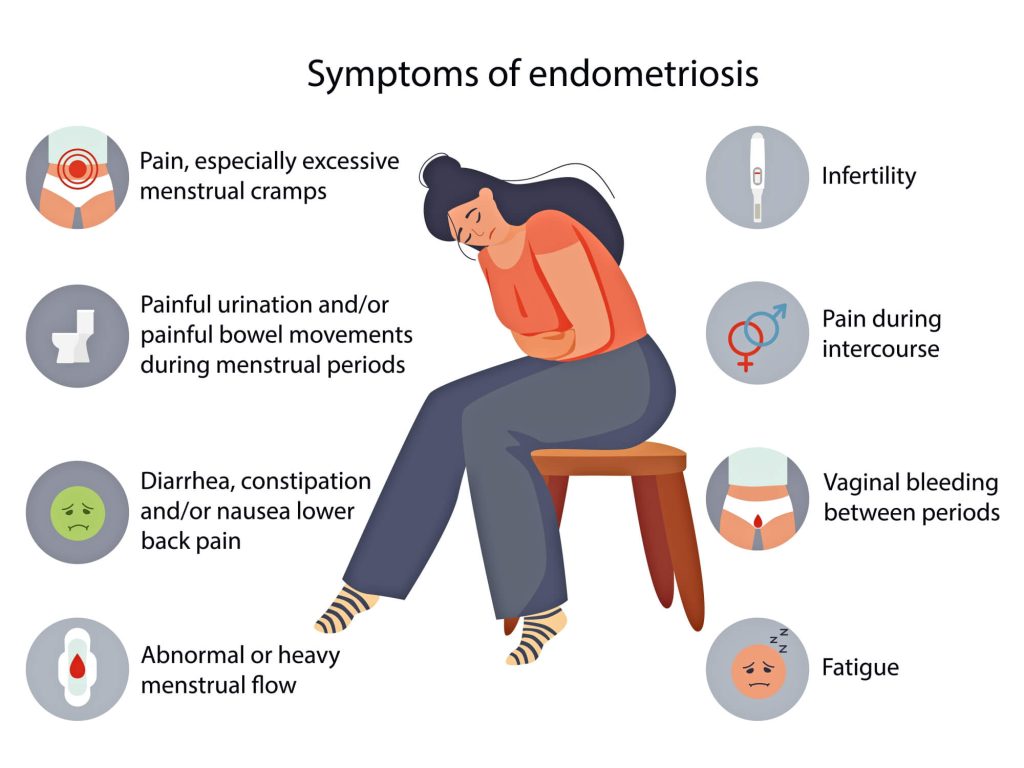
Fertility clinics see this pattern all the time. A patient arrives for an egg freezing consultation or a fertility workup, and their intake reveals classic symptoms of endometriosis: years of painful periods, chronic fatigue, pelvic pain, and infertility. By the time a patient is sitting in the exam room, the condition has been progressing unchecked for a decade or more.
Endometriosis affects roughly one in 10 women of reproductive age. The delay in diagnosis is a breakdown in care that leaves many to suffer in silence.
Why Endometriosis Stays Hidden
The average global diagnostic delay for endometriosis is close to seven years. In the U.S., estimates range from five to eight years, with some research placing it as high as 12. Up to 60% of cases may remain undiagnosed.
Menstrual cramps are the only type of pain society accepts as a normal phenomenon, which makes them easy for both patients and providers to dismiss with ibuprofen. Endometriosis symptoms overlap with irritable bowel syndrome (IBS), pelvic inflammatory disease, urinary tract infections (UTIs), and anxiety, leading to years of misdiagnosis.
Medical school curricula still dedicate minimal time to the condition. Until recently, the clinical standard required surgery to confirm a diagnosis. But you had to be in severe pain before anyone would operate, and you couldn’t get a diagnosis without the operation.
A 2025 study from Cornell and Weill Cornell Medicine analyzed over 30,000 posts across Reddit’s two largest endometriosis communities. “Medical professional” was the persona least associated with empathy in those forums. Patients feel most dismissed by the experts they rely on for help.
“I Thought It Was Just Bad Periods”
Melissa Diamond got her first period at 12. The pain was severe enough to keep her home from school. At 14, a gynecologist found a cyst on her ovary and surgically removed it. Melissa then spent nearly two decades seeking answers and being turned away.

She saw multiple gynecologists, raising the possibility of endometriosis or PCOS. Each time, Melissa was told she didn’t have those conditions and that birth control was the solution. She went back on the pill, but the symptoms continued.
It wasn’t until 2025—at age 33, more than 20 years after her symptoms began—that Melissa received a confirmed diagnosis. A pelvic MRI revealed endometriosis throughout her pelvis. Even though the condition doesn’t always appear on imaging, in Melissa’s case, the disease had become extensive enough to show up clearly. But it shouldn’t have taken two decades to order that scan.
For Melissa, like so many others, birth control was a double-edged sword. It masked her symptoms for decades but didn’t stop the endometriosis. When the pill is a catch-all solution rather than a diagnostic tool, the clock keeps ticking, often at the expense of a patient’s future fertility and well-being.
Silent Endometriosis and the Fertility Connection
Not every woman with endometriosis has painful periods. An estimated 20 to 25% of cases are completely asymptomatic. For these patients, infertility may be the first and only sign that something is wrong.
The clinical overlap between endometriosis and infertility is significant: 25-50% of women with infertility have endometriosis. The BCL6 biomarker, tested through an endometrial biopsy, is found in more than 50% of women with unexplained infertility. This suggests that many cases may have an identifiable cause providers aren’t testing for.
When a provider suspects silent endometriosis during a fertility workup at Extend, the evaluation may include a detailed pelvic exam, transvaginal ultrasound, and an endometrial biopsy to assess for inflammation. The goal is to identify what’s happening and have an honest conversation about what it means for the patient’s fertility options.
“Every Doctor Told Her Nothing Was Wrong”
Lisa, a 30-year-old Pilates instructor, had been on hormonal birth control for over a decade. When she stopped taking the pill at the end of 2020, her body responded within months. Pain shot from her ovaries down to her legs—a pain so intense she thought she might pass out.
Her gynecologist told her to come back in three months. Then three more months and three months after. Each time, providers told Lisa the cyst on her ovary would resolve on its own, but it didn’t. After the third visit, she refused to return and sought a second opinion.
Her eventual diagnosis: Stage 4 endometriosis. Lisa was relieved. She finally had proof that something was wrong, after being repeatedly told she was overreacting or that her symptoms were normal period pain.

Lisa’s story illustrates the second most common path to delayed diagnosis: active dismissal. She sought help and presented her symptoms clearly. But every visit ended the same way—with a provider defaulting to watchful waiting instead of investigation.
When a patient is repeatedly told that her pain isn’t real, she starts to doubt her own experience.
330,000 Stories of Systemic Failure—and How We Change the Narrative
For most, the road to an endometriosis diagnosis is a predictable cycle of frustration: years of worsening symptoms, a revolving door of providers, and a series of prescriptions that mask the symptoms without ever addressing the cause. Often, a specialist referral only comes once the pain is unbearable or the disease has taken a toll on a patient’s reproductive health.
Dr. Kathy Huang, director of NYU Langone’s Endometriosis Center, says endometriosis isn’t just a gynecological problem. It involves bowel health, bladder health, and mental health. A proper evaluation reveals the complexity and doesn’t start and end with a prescription for the pill.
Fortunately, the research is catching up to what patients have been saying for years. A 2025 study of 330,000 endometriosis patients found they had roughly double the odds of being diagnosed with an autoimmune condition—rheumatoid arthritis, lupus, Hashimoto’s—within two years of their diagnosis.
Researchers at Swansea University now argue the condition should be reclassified as a whole-body inflammatory disorder, not a reproductive one. The inflammatory proteins elevated in endometriosis patients are the same ones known to affect brain function and energy regulation, which means symptoms like fatigue, brain fog, and widespread pain aren’t exaggerations. They’re biological consequences of chronic inflammation that’s gone untreated.
A thorough fertility-focused evaluation includes a pelvic exam, transvaginal ultrasound, and sometimes biomarker testing to identify inflammation associated with endometriosis. It also includes something too many patients have never had: a direct conversation about findings, options, and timing.
If you’ve been told your pain is normal, that birth control is the only answer, or that nothing is wrong when you know it is, that’s a dismissal.
Validating the Years of Uncertainty
One woman, writing about her experience after 15 years of undiagnosed endometriosis, described her diagnosis as finding a missing page in the story of her life. She’d been through the ER visits, the misdiagnoses, and the doctors who labeled her ‘extra sensitive.’ When the answer finally came, she said it made her see every chapter of her life differently.
Early evaluation matters. Diagnostic tools exist today that didn’t a decade ago. The right provider won’t brush off what you’re feeling—they’ll investigate it until they have an answer.
If any of this sounds familiar, our providers are here to help you understand your reproductive health. Schedule a consultation and let’s discuss your options.


