What to Know About Endometriosis and Adenomyosis When Trying to Conceive
Both gynecological conditions involve abnormal growth of uterine-like tissue, but they affect different parts of the body. Here’s an overview of endometriosis and adenomyosis including symptoms, treatment, and how they can affect your fertility.
Here at the Extend Fertility office in New York City, we’re celebrating the arrival of great weather that spring brings. But March and April are also important months for the fertility community and for so many of our patients at Extend; March was Endometriosis Awareness Month and April is Adenomyosis Awareness Month, which aim to increase understanding about these gynecological conditions.
Both diseases involve abnormal growth of uterine-like tissue that can cause pelvic pain and infertility. However, they’re two separate diagnoses, each with their own set of challenges.
Here’s what to know about endometriosis and adenomyosis, from symptoms to diagnosis, to treatment, as well as how Extend Fertility can support you if you’re trying to conceive with both or either of these conditions.
WHAT IS ENDOMETRIOSIS?
Endometriosis is when the type of tissue that is supposed to live only in the lining of the uterus attaches to and grows in or on other nearby organs in the pelvis, including the ovaries, fallopian tubes, bowel, rectum and/or bladder. “Endo” as it is commonly known, is a chronic disease that can last from your first period until menopause, and can cause extreme pain, as well as infertility.
About 10 percent of women and girls of reproductive age have endometriosis and as many as 25 to 50 percent of women with infertility suffer from the disease. Experts don’t know why some of us have endo, and some don’t. One of the main theories is that instead of shedding the uterine lining through the vagina during a period, some of the tissue enters the pelvis and causes deposits of tissue to develop on surrounding tissue. These deposits can build up, making symptoms worse over time.
Sometimes, endometriosis can grow inside the ovary and form a cyst filled with dark brown fluid called an endometrioma, also known as a “chocolate cyst” due to its brownish appearance.
SYMPTOMS AND DIAGNOSIS OF ENDOMETRIOSIS
An estimated 20 to 25 percent of women with endometriosis have no symptoms, called silent endometriosis, which can make it harder to diagnose. But many women with endo experience intense symptoms, including:
- Menstrual pain, since the growths can react to hormone fluctuations
- Pain during sexual intercourse
- Pain with bowel movements
- Pain with urination
- Depression and anxiety
- Infertility
To diagnose endometriosis, your doctor will routinely perform both a pelvic exam and/or transvaginal ultrasound. If there is a high degree of suspicion for endo, and a definitive diagnosis might change decisions regarding the treatment plan (see below), your doctor might recommend laparoscopy – a minimally invasive surgery where the doctor will make three tiny incisions in the abdomen. They’ll insert a camera through one of the incisions to help visualize any potential lesions in the pelvis, and, if need be, remove them at the same time.
Laparoscopy is the gold standard and is required for a definitive endo diagnosis because it helps visualize the growths, as well as helps your doctor understand the severity of the disease. There are four stages of endometriosis, based on the amount, location and depth of the endometriosis that’s found during laparoscopy:
- Minimal endometriosis (Stage 1)
- Mild endometriosis (Stage 2)
- Moderate endometriosis (Stage 3)
- Severe endometriosis (Stage 4)
In some cases, your physician may also order special tests including a CT scan or an MRI to get a better look, or a specialized endometrial biopsy called ReceptivaDX.
ReceptivaDX FOR ENDOMETRIOSIS
Here at Extend Fertility, we do a full workup if we suspect you may have infertility caused by silent endometriosis, including running the ReceptivaDX test. We’ll take a sample of your endometrial tissue (via a minor procedure called an endometrial biopsy) and test for the presence of a marker called BCL6, which indicates inflammation in the uterus specific to endometriosis. The BCL6 marker is found in more than 50 percent of women with unexplained infertility and 65 percent of women with two or more failed IVF cycles.
If your ReceptivaDX results are negative, there’s a very good chance you don’t have endometriosis. If your results are positive this means uterine inflammation is present and you may have asymptomatic (silent) endometriosis.
It is important to note that this test suggests you have endo, but does not definitively diagnose you with the disease; as mentioned above, in cases where it is necessary to make a definitive diagnosis, a laparoscopy would need to be performed.
ENDOMETRIOSIS AND INFERTILITY
While the exact mechanisms of how endo can affect fertility are not totally clear, we do know that the inflammatory environment that is caused by endo can make it hard for an embryo to implant and can also affect egg quality. There’s also a link between endometriosis and ovulatory disorders, meaning you might not ovulate regularly, which can make getting pregnant more difficult.
Once you’ve been diagnosed, and/or if your ReceptivaDX result is positive, your Extend Fertility provider will offer any or all your options of treatment for endometriosis, depending on your specific case:
- Hormone treatment via an oral pill or hormone injection to suppress inflammation
- Laparoscopy or other surgery to remove the affected tissue
- Assisted reproductive technologies, such as IVF, to help with conception
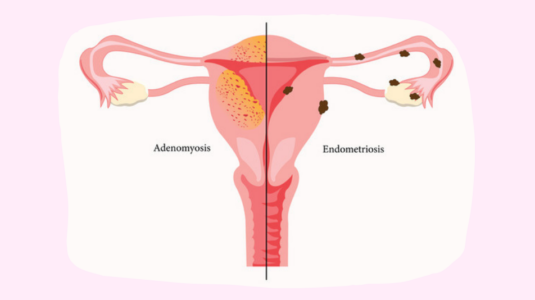
WHAT IS ADENOMYOSIS?
Adenomyosis is a similar disease to endometriosis in that it’s also a disease involving the type of cells that normally grow in the endometrial lining. But instead of the tissue growing outside the uterus as with endo, adenomyosis means the tissue grows into the myometrium, the muscular walls of the uterus.
Adenomyosis can lead to severe pain as the uterine walls thicken, break down and bleed with each menstrual cycle. The exact cause of adenomyosis is still unknown, and unfortunately, research on adenomyosis is limited when compared to other women’s health conditions.
Having one of these diseases does not mean you’ll have the other because they are two distinct conditions; but there is a correlation between the two. Research has found that adenomyosis might be present in about one third of women with surgically treated endometriosis, meaning they can appear simultaneously. Adenomyosis is typically diagnosed in women over the age of 40, whereas endometriosis is a lifelong condition that can start with your first-ever period.
ADENOMYOSIS SYMPTOMS AND INFERTILITY
One third of adenomyosis patients don’t have any symptoms, but the other two thirds will experience any or all the following symptoms:
- Heavy periods
- Pelvic pain
- Painful sex
- Severe back pain
- Bloating and discomfort
- Fatigue and anemia
- Enlarged uterus
- Infertility
Studies have found that adenomyosis can cause infertility by negatively impacting egg quality, embryo development, and implantation. Luckily, the use of assisted reproductive technology can help women with a diagnosis get pregnant and achieve a live birth.
TREATMENT FOR ENDOMETRIOSIS, ADENOMYOSIS AND INFERTILITY
Yes, you can still get pregnant with either or both of these challenging gynecologic conditions.
Controlled ovarian stimulation (COS) with intrauterine insemination (IUI), also known as superovulation, has been shown in studies to enhance fertility in women with endometriosis. Your reproductive endocrinologist will prescribe an oral medication like Clomid or Letrozole to produce follicle-stimulating hormone (FSH) and Luteinizing hormone (LH), which in turn will prompt your ovaries to release multiple eggs.
IVF followed by an embryo transfer also has great success rates for women with endo, up to about 42 percent per cycle for women under the age of 35.
If you have adenomyosis and are trying to conceive, treatment typically begins with hormonal medications to help with the pain and regulate menstrual cycle. In some cases, your provider may also suggest surgical excision to remove the disease, or other surgical options.
THE BOTTOM LINE
How your care team treats your endometriosis or adenomyosis will depend on your specific case. Your medical history, your history of infertility, your age, as well as your stage of disease will all be considered before establishing a treatment plan.
The good news is that though these conditions are not curable, both are treatable. It is possible to get pregnant if you have endometriosis or adenomyosis – it just means you might need a little help from assisted reproductive technologies and modern medicine.
And that’s where we come in. At Extend Fertility, we recognize the challenges faced by patients with endometriosis and adenomyosis and we’re here to provide education, support and options as you navigate your fertility journey.
Book a consultation today with one of Extend Fertility’s double board-certified providers. We won’t dismiss your pain; we’ll run the proper tests, provide a diagnosis if applicable and help you overcome your endo- or adeno-related infertility to help you grow your family on your terms.


