
PCOS is a hormone disorder that affects ovulation.
In order to understand PCOS, we need to first understand the normal function of the ovaries. The ovaries have a few major roles in the body. Firstly, they produce estrogen and progesterone, the hormones that help orchestrate the menstrual cycle and help build the uterine lining, as well as small amounts of “male” hormones called androgens, including testosterone.
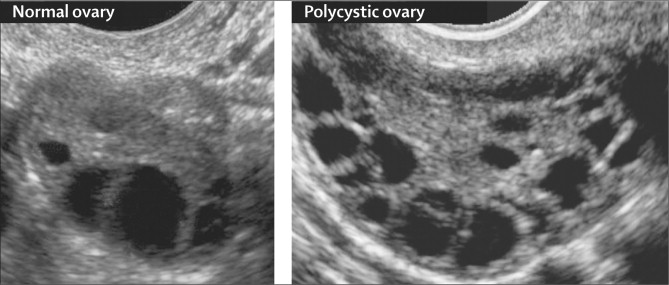
Secondly, the ovaries contain immature eggs, stored in sacs called “follicles,” and release one each cycle (typically each month). The process of maturing and releasing an egg for potential fertilization is called ovulation. If the egg isn’t fertilized, approximately two weeks after ovulation the body begins the process of menstruation—clearing out the uterine lining and the unfertilized egg so the ovaries can start again.
For patients with PCOS, this process is disrupted, resulting in two or three of the following symptoms:
- irregular or no periods, indicating irregular or no ovulation
- higher-than-normal androgen levels
- cysts in the ovaries that result from multiple cycles without ovulation (and may further affect ovarian function).
PCOS is really common.
In fact, it’s the most common endocrine (hormone) disorder in reproductive-age people with ovaries, affecting, conservatively, 5–10% of that population (some reports say up to 26%). PCOS is one of the leading causes of female fertility problems, responsible for an estimated 80% of “anovulatory” (no ovulation) infertility cases.
PCOS looks different for different people.
A diagnosis of PCOS is based on the presence of two of the three main indicators of PCOS, mentioned above (high androgens, irregular periods, polycystic ovaries). But there are many secondary symptoms, and the “picture of PCOS” looks very different for different patients. Common symptoms include:
- Heavy menstrual bleeding during the periods that do happen, because the uterine lining has built up for a longer period of time
- Excess hair growth, called hirsutism, because of the elevated androgens (over 70% of PCOS patients grow hair on their face and body, including back, belly, and chest)
- Acne on the face, chest, and upper back, again due to elevated androgen hormone levels
- Darkening of the skin, especially in creases such as the neck, groin, and under the breasts, called acanthosis nigricans
- Weight gain (up to 80% of women with PCOS are overweight or obese), which can exacerbate other PCOS symptoms
- Infertility
Not every PCOS patient will experience all, or even any, of these symptoms! This is part of the reason that PCOS is underdiagnosed—it’s so variable.
Doctors don’t know exactly what causes PCOS.
We know that PCOS tends to run in families. In one study of 52 families of PCOS patients, 58% of patients’ sisters also experienced PCOS symptoms. Researchers have tried to pinpoint one specific gene responsible for PCOS, but it’s more likely that many genes contribute to the condition.
Insulin resistance, which also runs in families, is closely associated with PCOS—but the relationship is not entirely clear. Insulin is a hormone produced by the pancreas that helps the body utilize sugar from food. If your body is resistant to insulin, you need higher levels of insulin to keep your blood sugar normal. Extra insulin in the bloodstream triggers the ovaries to produce more androgens.
Finally, there’s the relationship between obesity, insulin resistance, and PCOS—a real “chicken or the egg” situation. While insulin resistance and PCOS are known to cause weight gain, being obese or overweight also contributes to insulin resistance and PCOS. It’s not clear that obesity is a direct cause of PCOS, but research has shown that being overweight exacerbates the symptoms of PCOS, and that when overweight or obese PCOS patients lose weight, they experience fewer PCOS symptoms, can resume regular ovulation, and are better able to get pregnant (more on this later!).
Not every patient diagnosed with PCOS has elevated androgens or insulin resistance, or is obese or overweight. More research into the mechanisms behind PCOS is definitely necessary.
PCOS is associated with other health issues.
Actually, it’s the potential underlying cause of PCOS—insulin resistance—that contributes to most of the associated health problems. Two examples are type 2 diabetes and heart disease; the risk for both is increased in patients with insulin resistance. Additionally, PCOS and insulin resistance are associated with metabolic syndrome, a collection of risk factors (excess stomach fat, high triglyceride levels, low HDL cholesterol levels, high blood pressure, and high fasting blood sugar) that also contribute to diabetes, heart disease, and stroke.
Patients with PCOS who don’t have regular menstrual periods are at higher risk for a condition called endometrial hyperplasia, in which the lining of the uterus becomes too thick. Endometrial hyperplasia, in turn, increases the risk of endometrial cancer.
Sleep apnea, or repeated pauses in breathing during the night, is also associated with PCOS. Sleep apnea is more common in general for people who are overweight or obese, but PCOS also seems to contribute—the incidence of sleep apnea is higher in obese women with PCOS than in other obese women.
Treatment for PCOS depends on a patient’s symptoms and goals.
Like we mentioned, PCOS looks different for different patients. While there’s no cure, there are a few standard treatments, and which one your doctor prescribes will depend on your “PCOS picture” and your goals.
For patients who want to treat abnormal menstrual cycles and lower elevated androgens, which helps with hirsutism and acne, hormonal contraceptives like the pill are the “first-line” tool. Combined oral contraceptives (birth control pills containing both progesterone and estrogen) have been shown to lower testosterone levels and reduce PCOS symptoms.
For those trying to conceive, clomiphene (Clomid) or letrozole (Femara) are the go-to treatments. Clomiphene and letrozole are both medications that alter the estrogen levels to induce ovulation, and can be quite effective for PCOS patients—more on that below.
Many patients with PCOS are also prescribed metformin, a diabetes medication that increases insulin sensitivity. Metformin can treat some of the factors contributing to PCOS by lowering blood sugar and reducing the amount of insulin in the body. Like we explained above, higher insulin levels means higher androgen levels and increased weight gain, so lowering the level of insulin in the bloodstream may have a positive domino effect for PCOS patients.
PCOS can actually respond to lifestyle changes.
We’ve talked before about how eating healthfully and exercising isn’t necessarily a silver bullet for fertility; a healthy lifestyle can’t improve egg quality, and won’t extend your reproductive timeline. But for people with PCOS, certain lifestyle changes—namely, weight loss for obese or overweight patients—can actually make a big difference when it comes to managing symptoms and getting pregnant.
Research suggests that shedding between 5 and 10% of overall body weight can improve insulin resistance, reduce elevated androgen levels, improve ovulation and pregnancy rates, and reduce symptoms overall for overweight/obese patients with PCOS. Plus, weight loss can be extra effective alongside medical intervention. One study reported that obese/overweight patients taking clomiphene had an ovulation rate of 44.7% and a live birth rate of 10.2%; patients who paired treatment with a weight loss program had a 62% ovulation rate and a 25% live birth rate.
A few caveats: it’s not clear yet whether a specific diet is beneficial for PCOS patients, or whether exercise and diet together is better than one method alone. And weight loss isn’t the be-all, end-all of PCOS treatment; it hasn’t been shown to be useful for patients who are already a normal weight.
Pregnancy is totally possible with PCOS.
If you’ve been diagnosed with PCOS and you’re freaked out by everything you’ve read so far, we have some good news for you: PCOS doesn’t mean you won’t be able to get pregnant. Firstly, many people with PCOS ovulate sometimes, though it may be irregular (with cycles often lasting longer than 35 days). If there’s ovulation, there’s a chance at pregnancy—with PCOS, it may just take longer, because ovulation isn’t as frequent.
And even for patients with anovulation (no periods at all), treatment with low-cost oral medications like clomiphene or letrozole is usually very effective, and more complex and expensive infertility treatments like IVF typically aren’t required. Patients prescribed clomiphene or letrozole have been shown to have a pregnancy rate of 60–70% within six cycles.
Are you a PCOS patient trying to conceive? We can help.
Patients with PCOS can freeze their eggs, too!
People with PCOS typically don’t need IVF, but they may still consider egg freezing for the same reasons that other women do: because they want to proactively preserve their chance of pregnancy later in life. Interestingly, the characteristics of PCOS means that many women with this condition actually respond better to egg freezing than other women.
Firstly, women with PCOS often have higher anti-Müllerian levels; in fact, their AMH levels can be 2–3 times higher than women the same age without PCOS. AMH is an indicator of your egg count, and also serves as a good predictor of how many eggs you’ll be able to freeze in one cycle.
And that number, for people with PCOS, is typically higher, too. According to one study of IVF results for PCOS patients, women with PCOS had a “statistically significantly higher oocyte yield”—an average of 22.8 eggs per cycle, compared with the control group’s 16.5. The percentage of euploid (genetically healthy) embryos was the same between both groups, meaning that overall, women with PCOS ended up with a statistically significantly higher final number of healthy embryos from the eggs they froze.
Learn more about egg freezing.


