
Frequently asked fertility questions for National Infertility Awareness Week
It’s National Infertility Awareness Week, established in 1989 to increase public knowledge about infertility. NIAW hopes to promote discussion about fertility as a way to reduce misunderstanding and stigma, help those with infertility learn how to seek treatment, and help those at risk for infertility learn how to prevent it.
With that in mind, here are five frequently asked fertility questions, answered.
What is infertility?
Infertility is a disease of the reproductive system. Physicians define infertility as the inability to get or stay pregnant after 12 months of regular, unprotected sex. Being diagnosed as infertile doesn’t mean you can’t get pregnant ever. It just means something is preventing your body from getting pregnant on its own, and you may need to learn more about your cycle (such as when you’re ovulating) or get help from a fertility doctor, known as a reproductive endocrinologist, to understand and overcome the problem.
Learn more about defining infertility.
Is infertility common?
It’s probably more common than you think—experts estimate that 1 in 8 (or 12.5%) heterosexual, cisgender couples experience infertility. (“Social” infertility, meaning the inability to conceive due to non-medical factors, is also experienced by single people and LGBTQ couples.)
However, it’s important to note that infertility rates increase with age, with the steepest drop-off of fertility happening after age 35—which is why you’ll see that age thrown around a lot in conversations about fertility. According to the Office on Women’s Health at the U.S. Department of Health and Human Services, about one-third of women over age 35 experience infertility. That’s why, for women over 35, experts recommend seeing a doctor if they’re not pregnant after just 6 months of regular, unprotected sex. Even a half-year can make a difference.
What causes infertility?
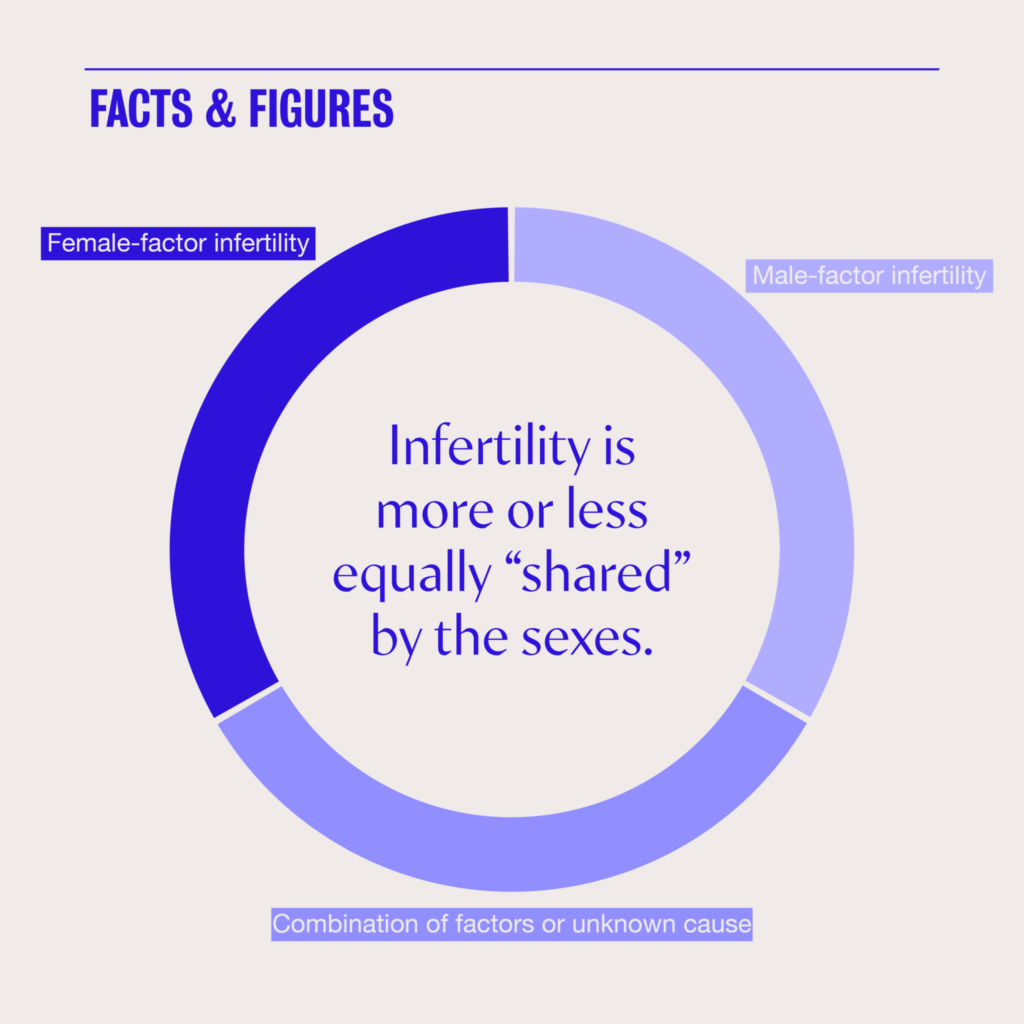
Infertility is more or less shared equally by the sexes: about a third of cases in hetero couples are deemed “female factor” infertility, another third are “male factor” infertility, and the final third is a combination of factors or an unknown issue.
For women, the most common cause of infertility is age. Women are born with all the eggs they’ll ever have, and as they age, both the quantity and the quality of those eggs declines. Egg quality refers to the number of eggs that are genetically “normal,” or free from chromosomal defects that could cause infertility, miscarriage, or congenital disorders. Both the decline in quantity, known as “diminished ovarian reserve,” and the decline in quality can affect a woman’s ability to get pregnant and give birth to a healthy baby.
Learn more about age and female fertility.
Age isn’t the only factor—certain disorders, imbalances, and uterine issues can also cause infertility, even in young women, and worsen fertility rates for older women. One example is endometriosis, a disorder of the endometrium (or uterine lining) that causes endometrial tissue to grow on other surfaces in the reproductive system, potentially causing cysts, blockages, or other barriers to normal reproductive function. Other possible causes include polycystic ovarian syndrome, or PCOS, smoking, and untreated sexually transmitted infections.
Learn more about what affects female fertility.
For men, age is a factor as well, although it’s less significant than it is for women. Age-related fertility decline starts a little later for men—around age 40—and the decline is just a few percentage points. However, if both partners are over 35, that decline can compound the woman’s declining fertility. Additionally, like we see in women’s eggs, chromosomal abnormalities are more likely to be present in sperm from men over 35 or 40.
Male infertility can be caused by a variety of factors: problems with sperm quality or count; varicocele, or a swelling of veins in the testicles; hormone imbalances; or problems with erection, ejaculation, or the tubes that carry sperm from the testicles to the penis. Like the female reproductive system, the male reproductive system has lots of moving parts, and they all have to work correctly for a pregnancy to happen.
Learn more about sperm & sperm health and male fertility decline.
What can I do now to prevent infertility later?
Because infertility is a natural result of age, there’s not a lot you can do to completely prevent it. The primary way to address potential future infertility is to freeze eggs, embryos, or sperm, known as fertility preservation. You might do this if you’re putting off childbearing to later in life (whether by choice or by circumstance), or if you plan to undergo a medical treatment that might impact your fertility, like cancer treatment or gender affirming hormones/surgery.
There are a few other things you can do to protect your fertility: If you’re a smoker, you can quit smoking, which can bring on menopause 1–4 years earlier. You can also make sure you get tested and promptly treated for sexually transmitted infections, as untreated STIs can cause pelvic inflammatory disease and potentially scarring in the reproductive system that may impede natural conception.
Men can improve their fertility by addressing lifestyle changes, such as smoking, diet, exercise, and any potential exposure to chemicals or toxins. Because sperm are created anew every day—as opposed to eggs, which are with us since birth—lifestyle changes can have a real impact on sperm health, and can often improve semen samples within 2–3 months.
Finally, while it won’t exactly prevent infertility, getting more information about your fertility early gives you more time, and more options, to address any potential problems. For women, this looks like a fertility assessment, with a hormone blood test and an ultrasound to estimate how many eggs you have and identify any uterine or ovarian issues. For men, the best test is a semen analysis—it measures the volume and chemistry of semen along with the concentration/count, motility (movement), and morphology (shape) of sperm.
What should I do if I think I’m experiencing infertility?
If you’ve been trying to conceive for 12 months if you’re under 35, 6 months if you’re over 35, or you have other barriers to conception (like known fertility issues or being in a same-sex couple), the best thing you can do is meet with a reproductive endocrinologist (a fertility specialist doctor). Typically, during or after a consultation, your doctor will order some additional testing that can guide them toward a diagnosis or a potential treatment.
A consultation doesn’t mean you need, or are obligated to start, infertility treatment. It’s simply the best way to get all the data you need to make a full informed choice about the next step in your fertility journey.


